Pharmacokinetic matching and mineralocorticoid adjustments · v1.2
Clinical Note: This calculator computes equivalent systemic glucocorticoid (anti-inflammatory) doses. It monitors for pharmacokinetic mismatches and loss of mineralocorticoid coverage.
1. Current Regimen
2. Target Regimen
Clinical Context & Pearls
Steroid conversions are not strictly linear. While standard equivalent tables provide a mathematical baseline, patient response varies based on receptor affinity, protein binding, and underlying organ dysfunction.
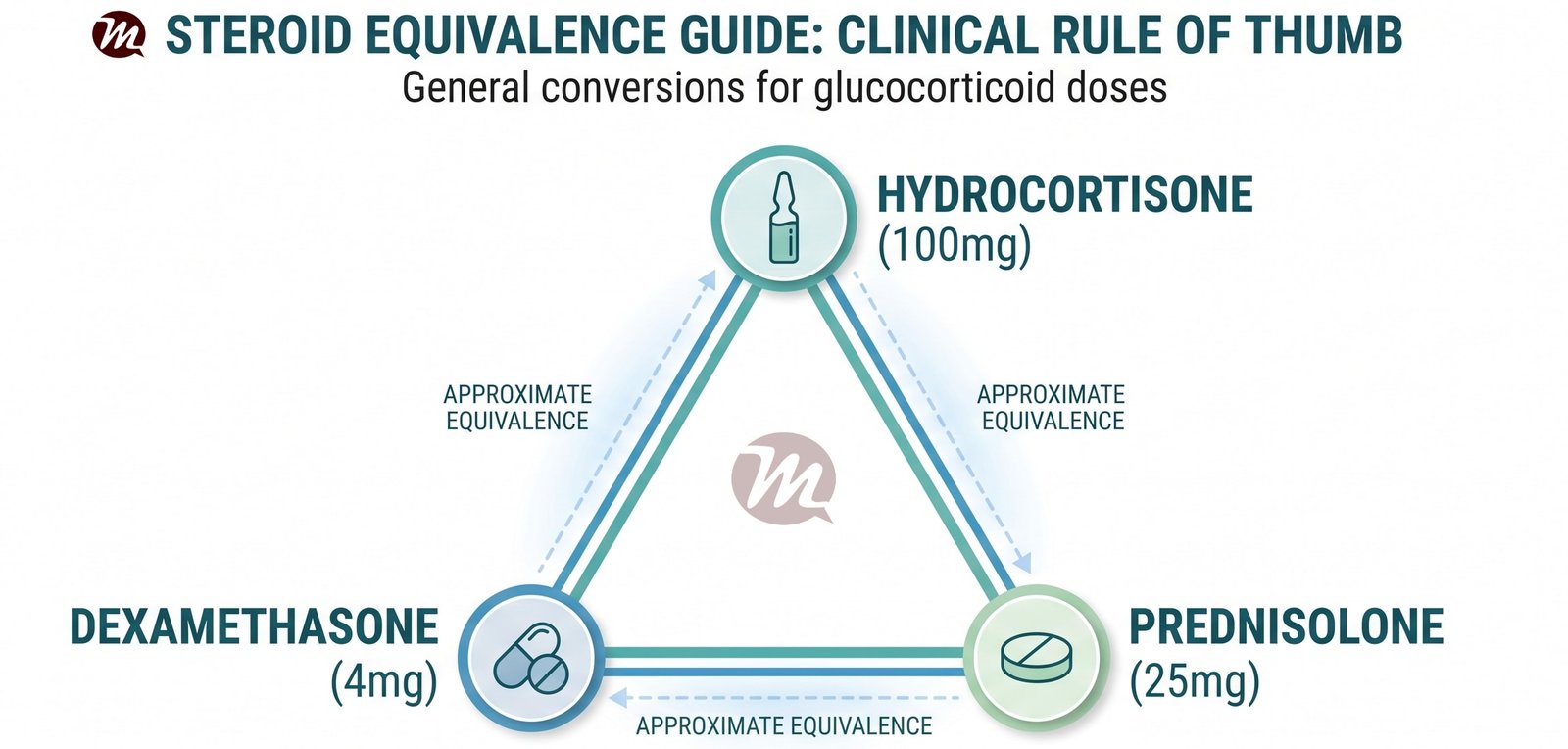
1. The 100-25-4 Equivalence Mnemonic
A clinical rule of thumb for standard glucocorticoid conversions.
A simple, commonly taught bedside mnemonic for estimating standard potency ratios is 100 = 25 x 4. This is highly useful during emergency resuscitation:
100 mg of Hydrocortisone (the physiological baseline) is roughly equivalent to...
25 mg of Prednisolone, which is roughly equivalent to...
4 mg of Dexamethasone. (Note: Strict pharmacological math places this closer to 3.75 mg, but 4 mg is the standard clinical approximation for this rule.)
1. Mineralocorticoid Activity (Sodium Retention)
The most dangerous error in steroid conversion is ignoring mineralocorticoid activity during critical illness (e.g., septic shock or Addisonian crisis).
Hydrocortisone has a 1:1 ratio of glucocorticoid to mineralocorticoid effect. It is the drug of choice for primary adrenal insufficiency.
Dexamethasone and Methylprednisolone have practically zero mineralocorticoid activity. If you switch a patient from Hydrocortisone to Dexamethasone, their blood pressure may collapse due to sodium wasting unless Fludrocortisone is added.
2. Biologic Half-Life & Dosing Frequency
You cannot convert a long-acting steroid to a short-acting steroid and maintain the same dosing frequency.
Short-acting (8-12 hours): Hydrocortisone, Cortisone. Must be dosed BID to QID.
Intermediate-acting (12-36 hours): Prednisolone, Methylprednisolone, Deflazacort. Can be dosed OD or BID.
Any patient on a dose greater than the physiological equivalent of 5 mg Prednisolone per day for more than 3 weeks must be assumed to have Hypothalamic-Pituitary-Adrenal (HPA) axis suppression.
Abrupt cessation will cause acute secondary adrenal insufficiency.
Tapering should be dictated by the underlying disease activity initially, but once below 7.5 mg of Prednisolone equivalent, the taper must slow significantly (e.g., 1 mg drop every 1-2 weeks) to allow the adrenal glands to recover physiological cortisol production.
5. Hepatic Impairment Note
Prednisone and Cortisone are inactive prodrugs that must be converted by the liver (via 11-beta-hydroxysteroid dehydrogenase) into active Prednisolone and Hydrocortisone. In patients with severe hepatic impairment, bypass the liver and prescribe Prednisolone or Hydrocortisone directly.
Abbreviations: GC (Glucocorticoid) · MC (Mineralocorticoid) · HPA (Hypothalamic-Pituitary-Adrenal) · OD (Once daily) · BID (Twice daily) · TDS/QID (Three/Four times daily)
Algorithm References & Evidence Base
Liu D, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30.
Paterno EM, et al. Glucocorticoid equivalence: a review of the literature. J Clin Endocrinol Metab. 2021.
UpToDate. Pharmacologic use of glucocorticoids. Accessed 2026.
How to Cite This Tool
AMA Style:
Umakanth S. Glucocorticoid Equivalence Converter. MEDiscuss. Published 2026. Accessed .
Vancouver Style:
Umakanth S. Glucocorticoid Equivalence Converter [Internet]. MEDiscuss.org; 2026 [cited ]. Available from:
CategoryTherapeutic Pathways & Algorithms
SpecialtiesInternal Medicine
StatusNew Pathway
Clinical content last reviewed: 29 July 2026 by Dr Shashikiran Umakanth